Micro Vascular Surgery


Replantation
Replantation is the surgical reattachment of a body part by microsurgical means, most commonly a finger, hand or arm, that has been completely cut from a person's body. Replantation of amputated parts has been performed on fingers, hands, forearms, arms, toes, feet, legs, ears, avulsed scalp injuries, a face, lips, penis and a tongue.
The first replantation peformed in the world with microvascular repair of vessels was done by a team of chief residents led by Dr. Ronald Malt at Massachusetts General Hospital in Boston, MA, USA in 1962. The arm of a 12 year old child severed at the level of the proximal humerus was reattached. The first report of a replantation published in a peer reviewed medical journal was reported by a team led by Zhong Wei Chen of the Sixth People's Hospital in Shanghai in 1963 writing in the Chinese Medical Journal. A machinist's hand was reattached at the level of the distal forearm. In this case vascular couplers were used for the vessels as the Chinese did not have good micro sutures available at that time. As there was little communication between China and the Western World in those years, Ronald Malt and Charles McKhann published in JAMA in 1964 their first two replantations without referencing the earlier published article from China.


Replantation requires microsurgery and must be performed within several hours of the part's amputation at a center with specialized equipment, surgeons and supporting staff. To improve the chances of a successful replantation, it is necessary to preserve the amputate as soon as possible in a cool(close to freezing, but not at or below freezing) and sterile or clean environment. Parts should be wrapped with moistened gauze and placed inside a clean or sterile bag floating in ice water. Dry ice should not be used as it can result in freezing of the tissue. There are so called sterile "Amputate-Bags" available which help to perform a dry, cool and sterile preservation.
Parts without muscles such as fingers can be preserved for many hours, while major muscled containing parts such as arms need to be re attached and revascularized within 6-8 hours to survive. Outcome of major limb replantations can be predicted by the potasium level of the blood which flows out of the replanted part after revascularization as a high level can be a marker of muscle and tissue death.
It is important to also collect and to preserve those amputates which do not look like being "replantable". A microsurgeon needs all available parts of human tissue to cover the wound at the stump and thus to prevent further shortening of the stump. In some cases (e.g. forearm) the task of an important joint (e.g. elbow) can be conserved for improved prosthetic success.
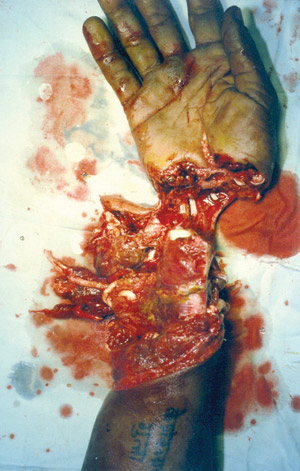
Severe crush injuries, multilevel injuries, avulsion injuries, and in some cases jagged tearing of tissue, can preclude replantation and salvage, requiring revision amputation of the stump. Severe crush injuries, multilevel injuries, avulsion injuries, and in some cases jagged tearing of tissue, can preclude replantation and salvage, requiring revision amputation of the stump. <